1
Introduction
1 min•119 words
Pre-Eclamptic Toxaemia (PET), widely referred to as preeclampsia, remains one of the primary drivers of maternal and perinatal morbidity and mortality worldwide (Sinkey et al., 2020). Developing typically after 20 weeks of gestation, it is characterized by new-onset hypertension and multi-system organ dysfunction, often manifesting as proteinuria or maternal endothelial injury (Sinkey et al., 2020).
Because there is no definitive cure for PET short of delivering the fetus and placenta, shifting the clinical paradigm toward primary prevention is crucial (Tong et al., 2021). Prophylactic use of low-dose aspirin (LDA) has emerged as a cornerstone, highly cost-effective intervention capable of reducing the incidence of preterm PET by more than 60% when properly initiated in at-risk populations (Ahn & Hwang, 2023).
Because there is no definitive cure for PET short of delivering the fetus and placenta, shifting the clinical paradigm toward primary prevention is crucial (Tong et al., 2021). Prophylactic use of low-dose aspirin (LDA) has emerged as a cornerstone, highly cost-effective intervention capable of reducing the incidence of preterm PET by more than 60% when properly initiated in at-risk populations (Ahn & Hwang, 2023).
2
Background & Pathophysiology
1 min•170 words
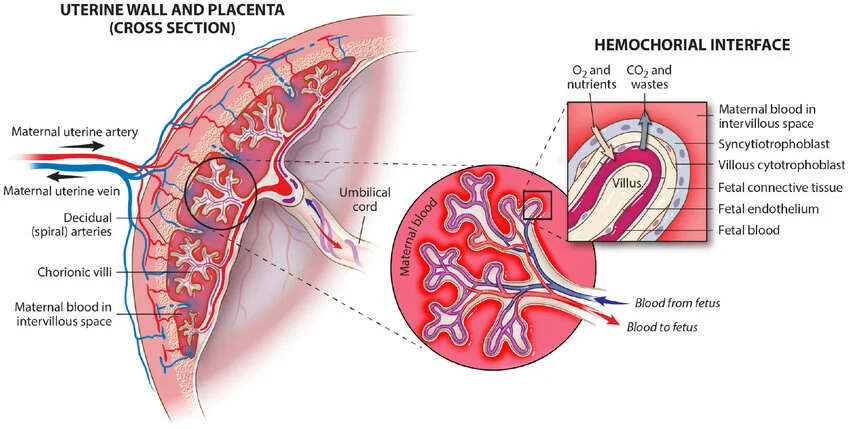
The physiological foundation of PET is rooted in abnormal placentation during early pregnancy (Tong et al., 2021).Impaired Remodeling: In a healthy pregnancy, trophoblasts invade the maternal uterine spiral arteries, transforming them from high-resistance, narrow vessels into low-resistance, high-caliber channels. In PET, this trophoblastic invasion is inadequate, leaving spiral arteries narrow and hyper-reactive (Tong et al., 2021).Ischemia & Imbalance: The resulting placental hypoperfusion creates local ischemia, triggering a massive release of antiangiogenic proteins and inflammatory cytokines into the maternal circulation (Tong et al., 2021). This processes disrupts the maternal vascular endothelial system.Mechanism of Aspirin: On a molecular level, PET causes a dysregulated maternal endothelial balance, tilting toward a high ratio of Thromboxane A2 (TXA2 - a potent vasoconstrictor and platelet aggregator) over Prostacyclin (PGI2 - a vasodilator). Low-dose aspirin (75–150 mg) selectively and irreversibly acetylates cyclooxygenase-1 (COX-1). This action suppresses the synthesis of Thromboxane A2 while sparing maternal Prostacyclin production, thereby restoring hemodynamic balance, preserving uteroplacental blood flow, and minimizing ischemia-related placental injury (Ahn & Hwang, 2023; Horgan et al., 2023)
3
Clinical Features
1 min•107 words
While aspirin prophylaxis is administered to prevent the disease, clinicians must remain vigilant for the signs and symptoms of developing PET during subsequent antenatal visits:Asymptomatic Sign: A significant, new elevation in blood pressure (Systolic >=140 mmHg or Diastolic ?=90 mmHg) after 20 weeks of gestation in a previously normotensive woman (Zhang & Wang, 2024).Severe Symptoms (End-Organ Damage):Severe, persistent, or worsening fronto-occipital headaches.Visual disturbances (e.g., blurring, flashing lights/scotomata, or double vision).Epigastric or right upper quadrant abdominal pain (due to hepatic swelling or Glisson's capsule stretch).Rapidly progressive edema, particularly sudden swelling of the face, hands, or feet, often accompanied by rapid weight gain.Altered mental status or hyperreflexia with clonus.
4
Diagnosis & Workup
2 min•328 words
Screening for pre-eclamptic toxaemia risk should ideally take place at the booking visit or early in the first trimester, before 16 weeks, using validated risk-stratification clinical criteria.
Identifying Candidates for Aspirin Prophylaxis
According to international clinical guidelines, low-dose aspirin should be prescribed if a pregnant woman presents with at least one high-risk factor or two or more moderate-risk factors.
High-risk factors where only one is required to start aspirin include:
Hypertensive disease in a previous pregnancy
Chronic kidney disease
Autoimmune diseases such as systemic lupus erythematosus or antiphospholipid syndrome
Pre-gestational Type 1 or Type 2 Diabetes Mellitus
Pre-existing chronic hypertension
Moderate-risk factors where two or more are required to start aspirin include:
First pregnancy, also known as nulliparity or being a primigravida
Advanced maternal age, specifically mothers aged 35 years or older
An interpregnancy interval of more than 10 years
Obesity, defined as a body mass index of 30 kilograms per square meter or higher at booking
A family history of pre-eclampsia in a mother or sister
Multi-fetal or twin gestation
Diagnostic Criteria for Established Pre-Eclamptic Toxaemia
If a patient advances past 20 weeks of gestation and is suspected of having pre-eclamptic toxaemia, the standard clinical diagnostic workup involves the following investigations:
Blood Pressure Measurement: Blood pressure must be checked using a correctly sized cuff, taken on two separate occasions at least 4 hours apart, showing a systolic blood pressure of 140 mmHg or higher, or a diastolic blood pressure of 90 mmHg or higher.
Proteinuria Assessment: This is confirmed via a urine dipstick reading of 2 plus or greater, a 24-hour urine collection tracking 300 milligrams of protein or more, or a random urine protein-to-creatinine ratio of 0.3 milligrams per milligram or higher.
Organ Dysfunction Labs: A full blood count is performed to check for thrombocytopenia or low platelets. Renal function tests are run to look for elevated creatinine, and liver function tests are conducted to check for transaminases raised to twice the upper limits of normal.
Identifying Candidates for Aspirin Prophylaxis
According to international clinical guidelines, low-dose aspirin should be prescribed if a pregnant woman presents with at least one high-risk factor or two or more moderate-risk factors.
High-risk factors where only one is required to start aspirin include:
Hypertensive disease in a previous pregnancy
Chronic kidney disease
Autoimmune diseases such as systemic lupus erythematosus or antiphospholipid syndrome
Pre-gestational Type 1 or Type 2 Diabetes Mellitus
Pre-existing chronic hypertension
Moderate-risk factors where two or more are required to start aspirin include:
First pregnancy, also known as nulliparity or being a primigravida
Advanced maternal age, specifically mothers aged 35 years or older
An interpregnancy interval of more than 10 years
Obesity, defined as a body mass index of 30 kilograms per square meter or higher at booking
A family history of pre-eclampsia in a mother or sister
Multi-fetal or twin gestation
Diagnostic Criteria for Established Pre-Eclamptic Toxaemia
If a patient advances past 20 weeks of gestation and is suspected of having pre-eclamptic toxaemia, the standard clinical diagnostic workup involves the following investigations:
Blood Pressure Measurement: Blood pressure must be checked using a correctly sized cuff, taken on two separate occasions at least 4 hours apart, showing a systolic blood pressure of 140 mmHg or higher, or a diastolic blood pressure of 90 mmHg or higher.
Proteinuria Assessment: This is confirmed via a urine dipstick reading of 2 plus or greater, a 24-hour urine collection tracking 300 milligrams of protein or more, or a random urine protein-to-creatinine ratio of 0.3 milligrams per milligram or higher.
Organ Dysfunction Labs: A full blood count is performed to check for thrombocytopenia or low platelets. Renal function tests are run to look for elevated creatinine, and liver function tests are conducted to check for transaminases raised to twice the upper limits of normal.
5
Management
2 min•217 words
The Prophylactic Regimen
Optimal Dose: Give low-dose aspirin at 150 mg daily (or a minimum of 75–81 mg depending on local resource availability, though landmark data like the ASPRE trial heavily favor 150 mg for superior reduction in preterm PET) (Ahn & Hwang, 2023).
Timing of Initiation: Aspirin must be started at 12 weeks of gestation (optimally between 12 and 16 weeks) (Tong et al., 2021). Initiating aspirin after 20 weeks yields significantly diminished therapeutic benefits because the primary window for spiral artery remodeling has already closed (Ahn & Hwang, 2023).
Administration: Instruct the patient to take the tablet nightly. Nocturnal administration is clinically proven to reduce nocturnal blood pressure surges more effectively than morning dosing.
Duration: Continue daily up to 36 weeks of gestation (or up to delivery if clinically indicated by specific local/institutional frameworks) (Tong et al., 2021). Discontinuing at 36 weeks is a common strategy to balance preeclampsia prevention with minimizing intrapartum or postpartum bleeding risks (Zhang & Wang, 2024).
Contraindications & Absolute Cautions
Before prescribing aspirin, a rigorous safety screening is mandatory. Avoid or exercise extreme caution in patients with:
Known hypersensitivity, allergy, or aspirin-induced asthma.
Active Peptic Ulcer Disease (PUD) or history of significant gastrointestinal bleeding.
Active bleeding disorders, thrombocytopenia, or concurrent use of other potent anticoagulants.
Severe hepatic or renal impairment.
Optimal Dose: Give low-dose aspirin at 150 mg daily (or a minimum of 75–81 mg depending on local resource availability, though landmark data like the ASPRE trial heavily favor 150 mg for superior reduction in preterm PET) (Ahn & Hwang, 2023).
Timing of Initiation: Aspirin must be started at 12 weeks of gestation (optimally between 12 and 16 weeks) (Tong et al., 2021). Initiating aspirin after 20 weeks yields significantly diminished therapeutic benefits because the primary window for spiral artery remodeling has already closed (Ahn & Hwang, 2023).
Administration: Instruct the patient to take the tablet nightly. Nocturnal administration is clinically proven to reduce nocturnal blood pressure surges more effectively than morning dosing.
Duration: Continue daily up to 36 weeks of gestation (or up to delivery if clinically indicated by specific local/institutional frameworks) (Tong et al., 2021). Discontinuing at 36 weeks is a common strategy to balance preeclampsia prevention with minimizing intrapartum or postpartum bleeding risks (Zhang & Wang, 2024).
Contraindications & Absolute Cautions
Before prescribing aspirin, a rigorous safety screening is mandatory. Avoid or exercise extreme caution in patients with:
Known hypersensitivity, allergy, or aspirin-induced asthma.
Active Peptic Ulcer Disease (PUD) or history of significant gastrointestinal bleeding.
Active bleeding disorders, thrombocytopenia, or concurrent use of other potent anticoagulants.
Severe hepatic or renal impairment.
6
Key Pearls & Takeaways
1 min•137 words
Early Action Saves Lives: Low-dose aspirin is a primary preventive tool; it must be started early (at 12 weeks, ideally before 16 weeks) to alter placental pathophysiology (Tong et al., 2021).
Dosing Matters: While 81 mg is traditional in some regions, contemporary global guidance strongly supports 150 mg nightly for maximizing risk reduction in high-risk categories without compromising safety (Ahn & Hwang, 2023; Horgan et al., 2023).
Risk Stratification: Do not wait for high blood pressure to develop. Evaluate risk factors (e.g., chronic HTN, DM, advanced maternal age, primigravida) at the very first antenatal booking to write the prescription timely (Sinkey et al., 2020).
Safety First: Always rule out active peptic ulcer disease, bleeding tendencies, or NSAID allergies prior to initiation. Stop the medication at 36 weeks to optimize hematological status for birth (Zhang & Wang, 2024).
Dosing Matters: While 81 mg is traditional in some regions, contemporary global guidance strongly supports 150 mg nightly for maximizing risk reduction in high-risk categories without compromising safety (Ahn & Hwang, 2023; Horgan et al., 2023).
Risk Stratification: Do not wait for high blood pressure to develop. Evaluate risk factors (e.g., chronic HTN, DM, advanced maternal age, primigravida) at the very first antenatal booking to write the prescription timely (Sinkey et al., 2020).
Safety First: Always rule out active peptic ulcer disease, bleeding tendencies, or NSAID allergies prior to initiation. Stop the medication at 36 weeks to optimize hematological status for birth (Zhang & Wang, 2024).
0/6