1
Introduction
1 min•123 words
A retained placenta is a major obstetric emergency and one of the primary drivers of severe primary postpartum hemorrhage, maternal shock, and sepsis worldwide. It is clinically defined as the failure of the placenta to deliver spontaneously within thirty minutes of birth during active management of the third stage of labor, or within sixty minutes with physiological management.
When the placenta remains trapped inside the uterine cavity, the myometrium cannot fully contract, preventing the uterine spiral arteries from sealing off. This results in rapid, life-threatening blood loss. The effective management of a retained placenta is a core Emergency Obstetric and Newborn Care skill. It must be executed with high precision by a skilled midwife or a medical doctor to prevent catastrophic maternal outcomes.
When the placenta remains trapped inside the uterine cavity, the myometrium cannot fully contract, preventing the uterine spiral arteries from sealing off. This results in rapid, life-threatening blood loss. The effective management of a retained placenta is a core Emergency Obstetric and Newborn Care skill. It must be executed with high precision by a skilled midwife or a medical doctor to prevent catastrophic maternal outcomes.
2
Background & Pathophysiology
1 min•184 words
The third stage of labor begins immediately after the delivery of the fetus and ends with the complete expulsion of the placenta and fetal membranes. Normal placental separation occurs due to the abrupt reduction in uterine surface area following fetal expulsion. This sudden shrinkage causes the placenta to buckle and detach from the decidual layer, forming a retroplacental hematoma that assists in completing the separation.
A retained placenta occurs through three main pathophysiological mechanisms: placenta adherens, where the myometrium fails to contract and shear off a normally separated placenta; a trapped placenta, where the placenta detaches completely but becomes incarcerated behind a partially closed cervix or a constriction ring; and placenta accreta spectrum, where abnormal trophoblastic invasion causes the placental villi to attach directly into or through the myometrium, lacking an intervening decidua basalis.
If the placenta is not removed, the uterine muscle remains in a state of atony. The open maternal blood vessels at the placental site continue to bleed heavily, leading to hypovolemic shock, consumptive coagulopathy, and an increased susceptibility to ascending bacterial infections due to an open cervix and retained tissue.
A retained placenta occurs through three main pathophysiological mechanisms: placenta adherens, where the myometrium fails to contract and shear off a normally separated placenta; a trapped placenta, where the placenta detaches completely but becomes incarcerated behind a partially closed cervix or a constriction ring; and placenta accreta spectrum, where abnormal trophoblastic invasion causes the placental villi to attach directly into or through the myometrium, lacking an intervening decidua basalis.
If the placenta is not removed, the uterine muscle remains in a state of atony. The open maternal blood vessels at the placental site continue to bleed heavily, leading to hypovolemic shock, consumptive coagulopathy, and an increased susceptibility to ascending bacterial infections due to an open cervix and retained tissue.
3
Clinical Features
1 min•158 words
Recognizing a retained placenta requires continuous tracking of the mother immediately following the birth of the baby.
The history of the current labor must be noted, including whether active management of the third stage was initiated, the timing of the delivery of the infant, and any history of retained placenta in previous pregnancies.
Physical examination focuses on assessing the classic signs of placental separation. These signs include a sudden gush of blood from the vagina, lengthening of the umbilical cord outside the vulva, and the uterus becoming firm, globular, and rising in the abdomen. If these signs are completely absent after thirty minutes of active management, a retained placenta is confirmed.
The clinician must look for features of maternal compromise, including tachycardia, hypotension, cold clammy extremities, worsening pallor, and visible or concealed ongoing vaginal bleeding. Assessing the contour of the uterus is also vital, as a hourglass-shaped uterus may signal a localized uterine constriction ring trapping the placenta.
The history of the current labor must be noted, including whether active management of the third stage was initiated, the timing of the delivery of the infant, and any history of retained placenta in previous pregnancies.
Physical examination focuses on assessing the classic signs of placental separation. These signs include a sudden gush of blood from the vagina, lengthening of the umbilical cord outside the vulva, and the uterus becoming firm, globular, and rising in the abdomen. If these signs are completely absent after thirty minutes of active management, a retained placenta is confirmed.
The clinician must look for features of maternal compromise, including tachycardia, hypotension, cold clammy extremities, worsening pallor, and visible or concealed ongoing vaginal bleeding. Assessing the contour of the uterus is also vital, as a hourglass-shaped uterus may signal a localized uterine constriction ring trapping the placenta.
4
Diagnosis & Workup
2 min•219 words
The diagnosis of a retained placenta is primarily clinical, based on the strict timeline of the third stage of labor. However, a rapid and targeted workup must be done concurrently to stabilize the mother and prepare for intervention.
Clinical Examination: Confirm the exact time of the delivery of the baby and verify that thirty minutes have passed. Palpate the abdomen to determine uterine tone, height, and the presence of a full bladder, which can mechanically displace the uterus and prevent placental delivery.
Vital Signs and Hemodynamic Assessment: Monitor blood pressure, pulse rate, respiratory rate, and oxygen saturation every five to ten minutes to catch early signs of hypovolemic shock.
Laboratory Evaluation: Draw blood immediately for a complete blood count to check baseline hemoglobin and hematocrit levels. Obtain a sample for blood typing, grouping, and cross-matching, as a blood transfusion is frequently required. If blood loss is massive, bedside clotting tests or a full coagulation profile should be initiated to check for disseminated intravascular coagulation.
Ultrasound Scan: Where available and if the patient is stable, a rapid bedside pelvic ultrasound can differentiate between a placenta that is completely detached but trapped, a partially separated placenta, and a placenta accreta spectrum. This helps the team avoid a forced manual removal that could trigger catastrophic hemorrhage in cases of deep invasive accreta.
Clinical Examination: Confirm the exact time of the delivery of the baby and verify that thirty minutes have passed. Palpate the abdomen to determine uterine tone, height, and the presence of a full bladder, which can mechanically displace the uterus and prevent placental delivery.
Vital Signs and Hemodynamic Assessment: Monitor blood pressure, pulse rate, respiratory rate, and oxygen saturation every five to ten minutes to catch early signs of hypovolemic shock.
Laboratory Evaluation: Draw blood immediately for a complete blood count to check baseline hemoglobin and hematocrit levels. Obtain a sample for blood typing, grouping, and cross-matching, as a blood transfusion is frequently required. If blood loss is massive, bedside clotting tests or a full coagulation profile should be initiated to check for disseminated intravascular coagulation.
Ultrasound Scan: Where available and if the patient is stable, a rapid bedside pelvic ultrasound can differentiate between a placenta that is completely detached but trapped, a partially separated placenta, and a placenta accreta spectrum. This helps the team avoid a forced manual removal that could trigger catastrophic hemorrhage in cases of deep invasive accreta.
5
Management
4 min•620 words
The management of a retained placenta demands an immediate, systematic procedure. It must progress logically from non-invasive physiological stimulation to mechanical extraction and postpartum stabilization.
Initial Non-Invasive Maneuvers: Begin by placing the newborn infant directly onto the mother's breast to suckle, or manually stimulate the mother's nipples. This tactile stimulation triggers the natural release of endogenous oxytocin from the posterior pituitary gland, promoting powerful uterine contractions. Ensure the mother's bladder is completely empty; if she cannot void, perform sterile urethral catheterization.
Controlled Cord Traction: Attempt controlled cord traction only when clear signs of placental separation are present. The clinician must stabilize the uterus abdominally by placing one hand over the suprapubic area, applying upward counter-traction, while the other hand applies gentle, steady downward traction on the umbilical cord. Avoid excessive or forceful traction on the cord under any circumstances, as it can break the cord, cause uterine inversion, or cause partial placental tearing.
Preparation for Manual Removal of the Placenta: If conservative measures fail and bleeding is ongoing, manual removal must be performed. Communication is vital; explain every stage of care to the mother at all times to gain her full cooperation, reduce anxiety, and secure her informed consent. Establish robust intravenous access with two large-bore cannulas and run intravenous fluids. Maintain strict aseptic technique throughout the procedure. Wash hands thoroughly and wear long, sterile gynecological gloves. Administer appropriate analgesia or sedation, such as intravenous ketamine, pethidine, or local pudendal block, depending on what you have available at the time, to manage severe pain and prevent neurogenic shock. Position the mother appropriately, ideally in the lithotomy position or with her knees flexed and thighs abducted, to make the vulva and uterus easily accessible.
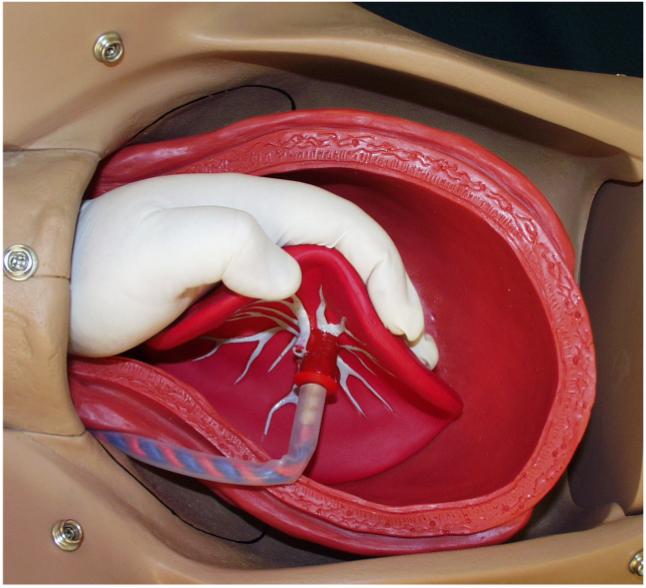
Intrauterine Extraction Procedure: Hold the umbilical cord with one hand to guide the way. Insert your other coned hand gently into the vagina and advance it up into the uterus, following the path of the umbilical cord if it is not broken, to locate the margin of the placenta. Once the placental edge is reached, use the side of your hand in a gentle, side-to-side sweeping movement, similar to using a wind-screen wiper, to cleanly shear and separate the placenta away from the uterine wall. Continue this sweeping motion until the entire placenta is detached. Gently grasp the complete placenta and remove it slowly from the uterine cavity. During this entire intrauterine maneuver, the external hand must firmly support the fundus of the uterus through the abdominal wall to provide counter-pressure, prevent uterine perforation, and stop the uterus from tearing away from its attachments.
Immediate Post-Removal Assessment: Once extracted, place the placenta on a flat surface and examine both the maternal cotyledons and the fetal membranes thoroughly for completeness. If any fragments or membranes are missing, re-explore the uterus to remove the retained tissue. If the mother is severely bleeding after removal, add another dose of uterotonics immediately. This includes administering twenty to forty units of oxytocin in an intravenous infusion, giving Ergometrine intramuscularly if not contraindicated by hypertension, or administering sublingual Misoprostol. If bleeding persists due to suspected trauma or fibrinolysis, administer intravenous Tranexamic acid within three hours of birth.
Postpartum Care and Monitoring: Continue monitoring the mother closely in the high-dependency area. Track vaginal bleeding, uterine contraction firmness, and maternal vital signs every fifteen minutes for the first two hours. Because manual entry into the uterine cavity introduces vaginal bacteria directly into the fundus, administer broad-spectrum prophylactic antibiotics appropriately to prevent endometritis and pelvic infection. If the placenta cannot be separated due to a suspected placenta accreta, or if life-threatening hemorrhage or complications arise that exceed facility capacity, stabilize the mother with intravenous fluids and rapidly refer her to a comprehensive emergency obstetric care center.
Initial Non-Invasive Maneuvers: Begin by placing the newborn infant directly onto the mother's breast to suckle, or manually stimulate the mother's nipples. This tactile stimulation triggers the natural release of endogenous oxytocin from the posterior pituitary gland, promoting powerful uterine contractions. Ensure the mother's bladder is completely empty; if she cannot void, perform sterile urethral catheterization.
Controlled Cord Traction: Attempt controlled cord traction only when clear signs of placental separation are present. The clinician must stabilize the uterus abdominally by placing one hand over the suprapubic area, applying upward counter-traction, while the other hand applies gentle, steady downward traction on the umbilical cord. Avoid excessive or forceful traction on the cord under any circumstances, as it can break the cord, cause uterine inversion, or cause partial placental tearing.
Preparation for Manual Removal of the Placenta: If conservative measures fail and bleeding is ongoing, manual removal must be performed. Communication is vital; explain every stage of care to the mother at all times to gain her full cooperation, reduce anxiety, and secure her informed consent. Establish robust intravenous access with two large-bore cannulas and run intravenous fluids. Maintain strict aseptic technique throughout the procedure. Wash hands thoroughly and wear long, sterile gynecological gloves. Administer appropriate analgesia or sedation, such as intravenous ketamine, pethidine, or local pudendal block, depending on what you have available at the time, to manage severe pain and prevent neurogenic shock. Position the mother appropriately, ideally in the lithotomy position or with her knees flexed and thighs abducted, to make the vulva and uterus easily accessible.
Intrauterine Extraction Procedure: Hold the umbilical cord with one hand to guide the way. Insert your other coned hand gently into the vagina and advance it up into the uterus, following the path of the umbilical cord if it is not broken, to locate the margin of the placenta. Once the placental edge is reached, use the side of your hand in a gentle, side-to-side sweeping movement, similar to using a wind-screen wiper, to cleanly shear and separate the placenta away from the uterine wall. Continue this sweeping motion until the entire placenta is detached. Gently grasp the complete placenta and remove it slowly from the uterine cavity. During this entire intrauterine maneuver, the external hand must firmly support the fundus of the uterus through the abdominal wall to provide counter-pressure, prevent uterine perforation, and stop the uterus from tearing away from its attachments.
Immediate Post-Removal Assessment: Once extracted, place the placenta on a flat surface and examine both the maternal cotyledons and the fetal membranes thoroughly for completeness. If any fragments or membranes are missing, re-explore the uterus to remove the retained tissue. If the mother is severely bleeding after removal, add another dose of uterotonics immediately. This includes administering twenty to forty units of oxytocin in an intravenous infusion, giving Ergometrine intramuscularly if not contraindicated by hypertension, or administering sublingual Misoprostol. If bleeding persists due to suspected trauma or fibrinolysis, administer intravenous Tranexamic acid within three hours of birth.
Postpartum Care and Monitoring: Continue monitoring the mother closely in the high-dependency area. Track vaginal bleeding, uterine contraction firmness, and maternal vital signs every fifteen minutes for the first two hours. Because manual entry into the uterine cavity introduces vaginal bacteria directly into the fundus, administer broad-spectrum prophylactic antibiotics appropriately to prevent endometritis and pelvic infection. If the placenta cannot be separated due to a suspected placenta accreta, or if life-threatening hemorrhage or complications arise that exceed facility capacity, stabilize the mother with intravenous fluids and rapidly refer her to a comprehensive emergency obstetric care center.
6
Key Pearls & Takeaways
1 min•157 words
Explaining Care Wins Trust: Always explain every stage of care to the mother at all times. Securing her cooperation and consent reduces pain perception and makes manual interventions significantly safer.
Never Pull a Fixed Cord: Avoid excessive traction on the umbilical cord. Pulling a placenta that has not separated can snap the cord, cause massive hemorrhage, or pull the uterus inside out, causing catastrophic uterine inversion.
Dual Hand Coordination: During manual removal, never insert your hand into the uterus without using your other hand to firmly support the uterus externally through the abdomen. This structural support is your primary shield against uterine perforation.
Verify the Placenta: Always inspect the delivered placenta and membranes for completeness. A single missing cotyledon left behind inside the uterus will cause ongoing postpartum hemorrhage and severe pelvic sepsis.
Prophylactic Antibiotics are Mandatory: Manual removal of a placenta is an invasive, unsterile-field procedure. Always administer broad-spectrum antibiotics post-procedure to prevent severe postpartum infections.
Never Pull a Fixed Cord: Avoid excessive traction on the umbilical cord. Pulling a placenta that has not separated can snap the cord, cause massive hemorrhage, or pull the uterus inside out, causing catastrophic uterine inversion.
Dual Hand Coordination: During manual removal, never insert your hand into the uterus without using your other hand to firmly support the uterus externally through the abdomen. This structural support is your primary shield against uterine perforation.
Verify the Placenta: Always inspect the delivered placenta and membranes for completeness. A single missing cotyledon left behind inside the uterus will cause ongoing postpartum hemorrhage and severe pelvic sepsis.
Prophylactic Antibiotics are Mandatory: Manual removal of a placenta is an invasive, unsterile-field procedure. Always administer broad-spectrum antibiotics post-procedure to prevent severe postpartum infections.
0/6