1
Introduction
1 min•123 words
Klebsiella pneumoniae has long been recognized as a major opportunistic pathogen responsible for severe nosocomial infections, particularly among immunocompromised patients in intensive care settings. However, the global epidemiology of this organism has drastically shifted with the emergence of a distinct clinical pathotype known as Hypervirulent Klebsiella pneumoniae (hvKp).
Unlike classic healthcare-associated strains, hypervirulent pathotypes are capable of causing severe, rapidly progressive, and life-threatening invasive infections in young, healthy, and completely immunocompetent individuals in the community. Originally described in the Asia-Pacific region, hvKp has now turned into a global public health threat.
The clinical hallmark of hvKp is its unique capacity for metastatic hematogenous seeding from a primary infection site to distant organs, leading to catastrophic multi-site empyemas, endophthalmitis, and central nervous system infections.
Unlike classic healthcare-associated strains, hypervirulent pathotypes are capable of causing severe, rapidly progressive, and life-threatening invasive infections in young, healthy, and completely immunocompetent individuals in the community. Originally described in the Asia-Pacific region, hvKp has now turned into a global public health threat.
The clinical hallmark of hvKp is its unique capacity for metastatic hematogenous seeding from a primary infection site to distant organs, leading to catastrophic multi-site empyemas, endophthalmitis, and central nervous system infections.
2
Background & Pathophysiology
2 min•213 words
To effectively manage this emerging pathogen, clinicians must understand the specific microbiological and molecular features that differentiate hypervirulent Klebsiella pneumoniae from classic healthcare-associated strains.
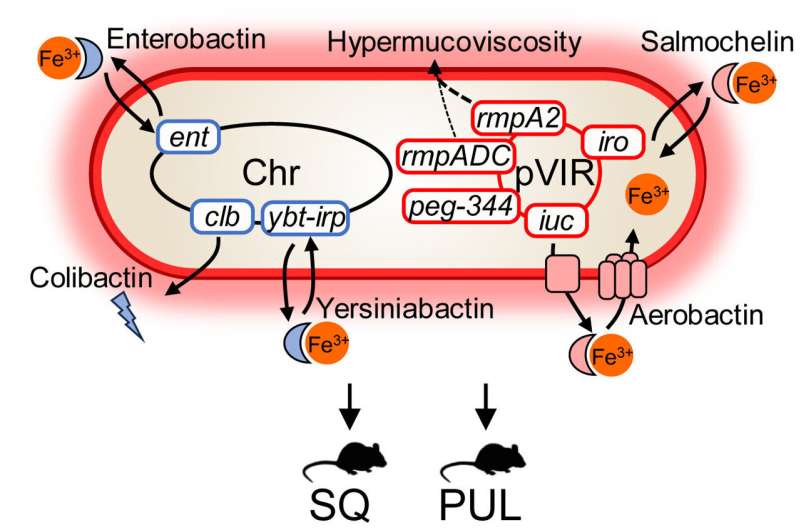
The hypervirulence pathotype is fundamentally driven by a distinct set of genetic virulence factors, typically carried on large virulence plasmids (such as pK2044 or pLVPK) or chromosomal genomic islands. These genetic elements drive a massive upregulation of capsule production, most frequently associated with the K1 and K2 capsular serotypes.
This hypermucoviscous capsule acts as a powerful shield, completely inhibiting complement-mediated killing and preventing neutrophil phagocytosis, allowing the bacteria to survive and replicate freely within the bloodstream.
Furthermore, hvKp strains secrete exceptionally high levels of specialized iron-scavenging molecules known as siderophores, specifically aerobactin and salmochelin. Because iron is a strictly limited resource within the human host, these high-affinity siderophores aggressively steal iron from host transport proteins like transferrin and lactoferrin. This supply of iron fuels rapid bacterial proliferation and enables the pathogen to cross tissue barriers, leading to widespread hematogenous dissemination and multi-organ abscess formation.
Alarmingly, while early hvKp strains were typically susceptible to most non-beta-lactam antibiotics, there is a rising convergence where hypervirulent strains are acquiring plasmid-mediated carbapenemases (such as KPC or NDM), giving rise to carbapenem-resistant hypervirulent Klebsiella pneumoniae (CR-hvKp), which combines extreme virulence with near-total antibiotic resistance.
The hypervirulence pathotype is fundamentally driven by a distinct set of genetic virulence factors, typically carried on large virulence plasmids (such as pK2044 or pLVPK) or chromosomal genomic islands. These genetic elements drive a massive upregulation of capsule production, most frequently associated with the K1 and K2 capsular serotypes.
This hypermucoviscous capsule acts as a powerful shield, completely inhibiting complement-mediated killing and preventing neutrophil phagocytosis, allowing the bacteria to survive and replicate freely within the bloodstream.
Furthermore, hvKp strains secrete exceptionally high levels of specialized iron-scavenging molecules known as siderophores, specifically aerobactin and salmochelin. Because iron is a strictly limited resource within the human host, these high-affinity siderophores aggressively steal iron from host transport proteins like transferrin and lactoferrin. This supply of iron fuels rapid bacterial proliferation and enables the pathogen to cross tissue barriers, leading to widespread hematogenous dissemination and multi-organ abscess formation.
Alarmingly, while early hvKp strains were typically susceptible to most non-beta-lactam antibiotics, there is a rising convergence where hypervirulent strains are acquiring plasmid-mediated carbapenemases (such as KPC or NDM), giving rise to carbapenem-resistant hypervirulent Klebsiella pneumoniae (CR-hvKp), which combines extreme virulence with near-total antibiotic resistance.
3
Clinical Features
1 min•198 words
The clinical presentation of hypervirulent Klebsiella pneumoniae is remarkably distinct from classic Klebsiella infections, presenting as a severe, community-acquired invasive syndrome rather than a localized hospital-acquired infection.
The primary presentation most frequently manifests as a solitary, large, community-acquired pyogenic liver abscess in a patient with no history of biliary tract disease or intra-abdominal pathology. Patients present with an acute onset of high-grade, swinging fevers, rigors, profound right upper quadrant abdominal pain, and marked constitutional symptoms.
The most defining and catastrophic clinical feature of hvKp is the phenomenon of spontaneous metastatic infection via hematogenous seeding. Even while a patient is undergoing therapy for a liver abscess, the bacteria can rapidly seed alternative sites, leading to:
Endogenous Endophthalmitis: Patients complain of sudden-onset ocular pain, progressive blurred vision, or a complete loss of vision. Physical examination reveals hypopyon, conjunctival injection, and rapid, irreversible destruction of the globe.
Central Nervous System Suppuration: Manifests as acute purulent meningitis or brain abscesses, causing neck stiffness, altered mental status, and focal neurological deficits.
Necrotizing Fasciitis and Soft Tissue Abscesses: Rapidly destructive, deep-tissue infections occurring spontaneously in the absence of documented external trauma.
Severe Pleuropulmonary Infections: Manifesting as necrotizing pneumonia, massive empyemas, and septic pulmonary emboli.
The primary presentation most frequently manifests as a solitary, large, community-acquired pyogenic liver abscess in a patient with no history of biliary tract disease or intra-abdominal pathology. Patients present with an acute onset of high-grade, swinging fevers, rigors, profound right upper quadrant abdominal pain, and marked constitutional symptoms.
The most defining and catastrophic clinical feature of hvKp is the phenomenon of spontaneous metastatic infection via hematogenous seeding. Even while a patient is undergoing therapy for a liver abscess, the bacteria can rapidly seed alternative sites, leading to:
Endogenous Endophthalmitis: Patients complain of sudden-onset ocular pain, progressive blurred vision, or a complete loss of vision. Physical examination reveals hypopyon, conjunctival injection, and rapid, irreversible destruction of the globe.
Central Nervous System Suppuration: Manifests as acute purulent meningitis or brain abscesses, causing neck stiffness, altered mental status, and focal neurological deficits.
Necrotizing Fasciitis and Soft Tissue Abscesses: Rapidly destructive, deep-tissue infections occurring spontaneously in the absence of documented external trauma.
Severe Pleuropulmonary Infections: Manifesting as necrotizing pneumonia, massive empyemas, and septic pulmonary emboli.
4
Diagnosis & Workup
2 min•277 words
A rapid, definitive laboratory and imaging workup must be initiated at the first sign of a suspected invasive Klebsiella infection to prevent permanent blindness or neurological devastation.
The String Test for Hypermucoviscosity: The definitive phenotypic screening tool for a suspected hvKp strain is the positive "string test" performed on a bacterial colony grown on an agar plate. Using a standard bacteriological inoculation loop, the clinician or microbiologist gently touches and lifts the colony. If the colony stretches and forms a continuous, viscous string measuring greater than five millimeters in length, the test is documented as positive for a hypermucoviscous phenotype.
Molecular and Genotypic Testing: While a positive string test is highly suggestive, definitive confirmation of an hvKp pathotype requires molecular testing via Polymerase Chain Reaction (PCR) to detect specific, plasmid-borne virulence genes. The presence of the aerobactin biosynthesis gene (iucA), the regulator of mucoid phenotype genes (rmpA and rmpA2), or specific capsular serotype genes (K1 and K2) serves as the gold standard confirmation.
Complete Microbiological and Biochemical Profile: Order immediate, multiple sets of blood cultures alongside high-quality aspirates or cultures from the primary abscess fluid. Request an immediate complete blood count, which typically demonstrates a profound leukocytosis, and baseline biochemical markers including markedly elevated C-Reactive Protein and Procalcitonin.
Diagnostic and Surveillance Imaging: Request an urgent ultrasound or contrast-enhanced Computed Tomography (CT) scan of the abdomen to map the primary pyogenic liver abscess. Crucially, due to the high rate of metastatic seeding, the discovery of a Klebsiella liver abscess must immediately trigger a comprehensive imaging and clinical survey, including a chest CT to rule out septic emboli and an immediate ophthalmological evaluation if any visual changes are reported.
The String Test for Hypermucoviscosity: The definitive phenotypic screening tool for a suspected hvKp strain is the positive "string test" performed on a bacterial colony grown on an agar plate. Using a standard bacteriological inoculation loop, the clinician or microbiologist gently touches and lifts the colony. If the colony stretches and forms a continuous, viscous string measuring greater than five millimeters in length, the test is documented as positive for a hypermucoviscous phenotype.
Molecular and Genotypic Testing: While a positive string test is highly suggestive, definitive confirmation of an hvKp pathotype requires molecular testing via Polymerase Chain Reaction (PCR) to detect specific, plasmid-borne virulence genes. The presence of the aerobactin biosynthesis gene (iucA), the regulator of mucoid phenotype genes (rmpA and rmpA2), or specific capsular serotype genes (K1 and K2) serves as the gold standard confirmation.
Complete Microbiological and Biochemical Profile: Order immediate, multiple sets of blood cultures alongside high-quality aspirates or cultures from the primary abscess fluid. Request an immediate complete blood count, which typically demonstrates a profound leukocytosis, and baseline biochemical markers including markedly elevated C-Reactive Protein and Procalcitonin.
Diagnostic and Surveillance Imaging: Request an urgent ultrasound or contrast-enhanced Computed Tomography (CT) scan of the abdomen to map the primary pyogenic liver abscess. Crucially, due to the high rate of metastatic seeding, the discovery of a Klebsiella liver abscess must immediately trigger a comprehensive imaging and clinical survey, including a chest CT to rule out septic emboli and an immediate ophthalmological evaluation if any visual changes are reported.
5
Management
2 min•294 words
The management of hypervirulent Klebsiella pneumoniae must be immediate, aggressive, and multi-disciplinary, integrating optimized intravenous antimicrobial therapy with timely source control.
Targeted Intravenous Antimicrobial Therapy: Because hvKp infections are community-acquired, empiric therapy in a critically ill patient must be broad enough to cover standard Gram-negative rods while accounting for potential beta-lactamase production. Initial empiric therapy should consist of a high-dose, broad-spectrum carbapenem, such as Intravenous Meropenem (1g to 2g administered every 8 hours) or Intravenous Imipenem, or a fourth-generation cephalosporin such as Cefepime.
Once definitive antimicrobial susceptibility testing confirms that the strain is fully susceptible and does not harbor extended-spectrum beta-lactamases (ESBLs) or carbapenemases, therapy can be safely narrowed to a third-generation cephalosporin, such as Intravenous Ceftriaxone (2g administered every 12 to 24 hours).
For strains identified as carbapenem-resistant hypervirulent Klebsiella pneumoniae (CR-hvKp), treatment options are severely limited and require combination therapy utilizing novel beta-lactam/beta-lactamase inhibitors like Ceftazidime-Avibactam, or combining Colistin or Plazomicin with high-dose carbapenem infusions based on minimum inhibitory concentration profiles. Intravenous therapy must be maintained for at least 3 to 4 weeks for uncomplicated liver abscesses, and extended up to 6 weeks or longer for complex metastatic collections or osteomyelitis.
Aggressive Source Control and Drainage: Antimicrobial therapy alone is structurally insufficient to clear large, walled-off purulent collections. Any pyogenic liver abscess or large fluid collection measuring greater than 3 to 5 centimeters must undergo immediate image-guided percutaneous needle aspiration or the placement of a continuous pigtail drainage catheter.
Emergency Management of Endophthalmitis: If the patient develops signs of endogenous endophthalmitis, this represents a profound medical emergency. An immediate ophthalmological consultation must be secured for the urgent intravitreal injection of antibiotics (such as Intravitreal Vancomycin combined with Ceftazidime) alongside prompt consideration for an emergency pars plana vitrectomy to save the patient's vision.
Targeted Intravenous Antimicrobial Therapy: Because hvKp infections are community-acquired, empiric therapy in a critically ill patient must be broad enough to cover standard Gram-negative rods while accounting for potential beta-lactamase production. Initial empiric therapy should consist of a high-dose, broad-spectrum carbapenem, such as Intravenous Meropenem (1g to 2g administered every 8 hours) or Intravenous Imipenem, or a fourth-generation cephalosporin such as Cefepime.
Once definitive antimicrobial susceptibility testing confirms that the strain is fully susceptible and does not harbor extended-spectrum beta-lactamases (ESBLs) or carbapenemases, therapy can be safely narrowed to a third-generation cephalosporin, such as Intravenous Ceftriaxone (2g administered every 12 to 24 hours).
For strains identified as carbapenem-resistant hypervirulent Klebsiella pneumoniae (CR-hvKp), treatment options are severely limited and require combination therapy utilizing novel beta-lactam/beta-lactamase inhibitors like Ceftazidime-Avibactam, or combining Colistin or Plazomicin with high-dose carbapenem infusions based on minimum inhibitory concentration profiles. Intravenous therapy must be maintained for at least 3 to 4 weeks for uncomplicated liver abscesses, and extended up to 6 weeks or longer for complex metastatic collections or osteomyelitis.
Aggressive Source Control and Drainage: Antimicrobial therapy alone is structurally insufficient to clear large, walled-off purulent collections. Any pyogenic liver abscess or large fluid collection measuring greater than 3 to 5 centimeters must undergo immediate image-guided percutaneous needle aspiration or the placement of a continuous pigtail drainage catheter.
Emergency Management of Endophthalmitis: If the patient develops signs of endogenous endophthalmitis, this represents a profound medical emergency. An immediate ophthalmological consultation must be secured for the urgent intravitreal injection of antibiotics (such as Intravitreal Vancomycin combined with Ceftazidime) alongside prompt consideration for an emergency pars plana vitrectomy to save the patient's vision.
6
Key Pearls & Takeaways
1 min•173 words
Key Pearls and Takeaways
Community-Acquired but Deadly: Never assume that a severe Klebsiella infection is purely a hospital-acquired issue. A young, healthy patient presenting from the community with a massive liver abscess is the classic presentation of Hypervirulent Klebsiella pneumoniae.
Starch and String Test: The string test is a rapid, zero-cost phenotypic indicator. If a Klebsiella culture stretches more than five millimeters on an inoculation loop, immediately escalate your clinical suspicion for a hypervirulent pathotype.
Hunt for Metastatic Lesions: A diagnosis of an hvKp liver abscess must never be treated as a localized infection. Actively search the eyes, lungs, and central nervous system for hidden, spontaneous bacterial seeding.
The Vision Crisis: Endogenous endophthalmitis driven by hvKp can cause complete, permanent blindness within 24 to 48 hours of ocular symptom onset. Any visual complaint requires emergency intravitreal antibiotic deployment.
The Convergent Nightmare: The modern evolution of hvKp combining hypervirulence with carbapenem resistance (CR-hvKp) represents one of the most challenging therapeutic scenarios in modern infectious disease medicine, demanding immediate combination therapy and strict contact isolation.
Community-Acquired but Deadly: Never assume that a severe Klebsiella infection is purely a hospital-acquired issue. A young, healthy patient presenting from the community with a massive liver abscess is the classic presentation of Hypervirulent Klebsiella pneumoniae.
Starch and String Test: The string test is a rapid, zero-cost phenotypic indicator. If a Klebsiella culture stretches more than five millimeters on an inoculation loop, immediately escalate your clinical suspicion for a hypervirulent pathotype.
Hunt for Metastatic Lesions: A diagnosis of an hvKp liver abscess must never be treated as a localized infection. Actively search the eyes, lungs, and central nervous system for hidden, spontaneous bacterial seeding.
The Vision Crisis: Endogenous endophthalmitis driven by hvKp can cause complete, permanent blindness within 24 to 48 hours of ocular symptom onset. Any visual complaint requires emergency intravitreal antibiotic deployment.
The Convergent Nightmare: The modern evolution of hvKp combining hypervirulence with carbapenem resistance (CR-hvKp) represents one of the most challenging therapeutic scenarios in modern infectious disease medicine, demanding immediate combination therapy and strict contact isolation.
0/6