1
Introduction
1 min•109 words
Recurrent Pregnancy Loss (RPL) is a profoundly challenging clinical entity that carries an immense emotional and psychological burden for patients and families. Historically defined by three or more consecutive pregnancy losses, modern consensus guidelines have shifted the investigative landscape, lowering the threshold to optimize early detection and intervention.
Managing RPL demands a highly disciplined, evidence-based approach. Because the etiologies of pregnancy loss are multifactorial—ranging from structural uterine anomalies and autoimmune disruptions to genetic factors—clinicians must strictly separate mandatory, high-yield diagnostic investigations from low-yield, non-routine testing panels. Furthermore, acute management must rely on proven pharmacological therapies, deliberately avoiding expensive and unproven experimental interventions in favor of protocolized, supportive clinical care.
Managing RPL demands a highly disciplined, evidence-based approach. Because the etiologies of pregnancy loss are multifactorial—ranging from structural uterine anomalies and autoimmune disruptions to genetic factors—clinicians must strictly separate mandatory, high-yield diagnostic investigations from low-yield, non-routine testing panels. Furthermore, acute management must rely on proven pharmacological therapies, deliberately avoiding expensive and unproven experimental interventions in favor of protocolized, supportive clinical care.
2
Background & Pathophysiology
1 min•199 words
The biological process of maintaining a successful early pregnancy requires a flawless orchestration of embryonic chromosomal integrity, adequate structural anatomy, balanced endocrine support, and local maternal immunotolerance. Recurrent pregnancy loss occurs when one or more of these critical homeostatic mechanisms are disrupted.
The primary pathological mechanisms driving RPL include:
1. Anatomical Distortions: Congenital uterine anomalies (such as a septate or bicornuate uterus) or acquired structural lesions (such as submucosal leiomyomas or intrauterine adhesions) alter the architecture of the endometrial cavity. This directly compromises local vascular sub-endothelial perfusion, preventing normal blastocyst implantation or restricting mid-trimester gestational expansion.
2. Autoimmune Thrombotic Microangiopathy: Antiphospholipid Syndrome (APS) represents the most definitive, treatable autoimmune cause of RPL. Maternal autoantibodies target phospholipid-binding plasma proteins, directly inducing a pro-thrombotic state. This triggers microvascular thrombosis, placental infarction, and defective trophoblast invasion within the developing uteroplacental circulation, causing early or mid-trimester embryonic death.
3. Luteal Phase and Endocrine Insufficiency: Adequate progesterone secretion from the corpus luteum is absolutely mandatory during the first 7 to 9 weeks of gestation to maintain endometrial decidualization and structural uterine quiescence. True luteal phase deficiency or blunted progesterone receptor sensitivity starves the early gestational sac of necessary hormonal support, leading to premature detachment.
The primary pathological mechanisms driving RPL include:
1. Anatomical Distortions: Congenital uterine anomalies (such as a septate or bicornuate uterus) or acquired structural lesions (such as submucosal leiomyomas or intrauterine adhesions) alter the architecture of the endometrial cavity. This directly compromises local vascular sub-endothelial perfusion, preventing normal blastocyst implantation or restricting mid-trimester gestational expansion.
2. Autoimmune Thrombotic Microangiopathy: Antiphospholipid Syndrome (APS) represents the most definitive, treatable autoimmune cause of RPL. Maternal autoantibodies target phospholipid-binding plasma proteins, directly inducing a pro-thrombotic state. This triggers microvascular thrombosis, placental infarction, and defective trophoblast invasion within the developing uteroplacental circulation, causing early or mid-trimester embryonic death.
3. Luteal Phase and Endocrine Insufficiency: Adequate progesterone secretion from the corpus luteum is absolutely mandatory during the first 7 to 9 weeks of gestation to maintain endometrial decidualization and structural uterine quiescence. True luteal phase deficiency or blunted progesterone receptor sensitivity starves the early gestational sac of necessary hormonal support, leading to premature detachment.
3
Clinical Features
1 min•68 words
Establishing a precise clinical history is the first critical step in evaluating a patient presenting with pregnancy loss. The clinician must document the exact gestational age of each previous loss, the presence or absence of a fetal heartbeat prior to cessation, a history of concurrent autoimmune symptoms (such as joint pain, malar rash, or previous unprovoked deep vein thromboses), and any family history of structural or genetic abnormalities.
3.1
1. Timeline for Initial Investigation
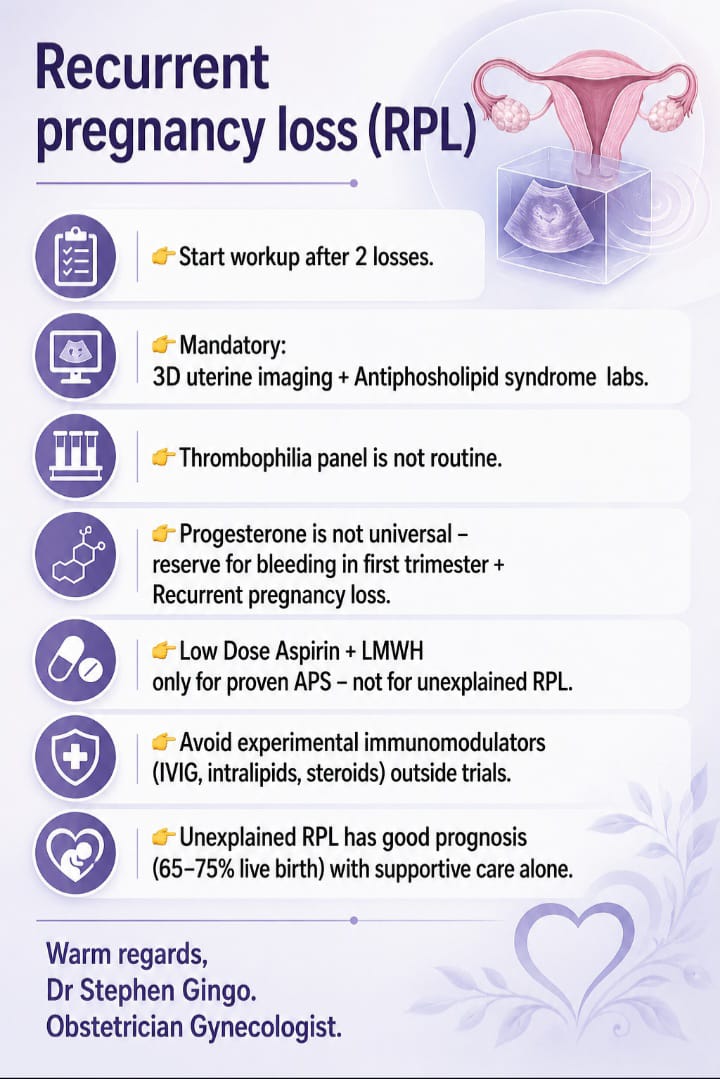
A critical clinical pearl in modern gynecology is the timing of the diagnostic workup. Rather than waiting for the classic threshold of three consecutive miscarriages, clinicians must actively initiate a formal RPL workup after 2 consecutive pregnancy losses. Early investigation prevents predictable, recurrent reproductive failures and offers reassurance to the patient.
3.2
2. Monitoring and Prognosis
Patients with a history of RPL who conceive again require close monitoring. However, clinicians must counsel couples that even when an exhaustive workup yields no definitive cause—classified as Unexplained RPL—the baseline prognosis remains highly favorable. With close clinical monitoring and structured, compassionate supportive care alone, unexplained RPL carries an excellent prognosis, yielding a 65% to 75% live birth rate in subsequent pregnancies.
4
Diagnosis & Workup
1 min•31 words
The diagnostic workup for recurrent pregnancy loss must be highly structured, focusing strictly on mandatory, high-yield investigations while actively omitting unnecessary screening panels that add financial strain without altering clinical management.
4.1
1. Mandatory Anatomical and Autoimmune Investigations
Every standard RPL workup must include two foundational pillars:
- Advanced 3D Uterine Imaging: Evaluating the structural configuration of the uterine cavity is mandatory. This is achieved using 3D transvaginal ultrasound, hysterosalpingography (HSG), or saline infusion sonohysterography to accurately identify or rule out a septate uterus, sub-mucosal fibroids, or congenital mullerian defects.
- Antiphospholipid Syndrome (APS) Serology: Screening for APS is mandatory. Clinicians must order a comprehensive serological panel checking for Lupis Anticoagulant, Anti-beta-2-glycoprotein I (IgG/IgM), and Anti-cardiolipin antibodies (IgG/IgM). To confirm a true diagnosis of APS, positive serological titers must be documented on two separate occasions at least 12 weeks apart.
- Advanced 3D Uterine Imaging: Evaluating the structural configuration of the uterine cavity is mandatory. This is achieved using 3D transvaginal ultrasound, hysterosalpingography (HSG), or saline infusion sonohysterography to accurately identify or rule out a septate uterus, sub-mucosal fibroids, or congenital mullerian defects.
- Antiphospholipid Syndrome (APS) Serology: Screening for APS is mandatory. Clinicians must order a comprehensive serological panel checking for Lupis Anticoagulant, Anti-beta-2-glycoprotein I (IgG/IgM), and Anti-cardiolipin antibodies (IgG/IgM). To confirm a true diagnosis of APS, positive serological titers must be documented on two separate occasions at least 12 weeks apart.
4.2
2. Inappropriate and Non-Routine Testing
Thrombophilia Panels: Running a routine hereditary thrombophilia panel (such as testing for Factor V Leiden, Prothrombin gene mutations, or Protein C and S deficiencies) is not routinely recommended for patients with recurrent pregnancy loss. Evidence demonstrates that screening for inherited thrombophilias does not alter the clinical outcome or predict therapeutic success in subsequent pregnancies, and should be strictly reserved for patients with a personal, unprovoked history of systemic thromboembolism.
5
Management
1 min•18 words
Therapeutic interventions in RPL must be driven by definitive diagnostic indicators rather than empiric or speculative medical management.
5.1
1. Targeted Management for Proven Antiphospholipid Syndrome
Pharmacological therapy using a combination of Low-Dose Aspirin (75–100 mg daily) and Low-Molecular-Weight Heparin (LMWH) is highly effective and mandatory, but its use must be strictly restricted. This combination therapy is indicated only for patients with a laboratory-proven diagnosis of Antiphospholipid Syndrome. Administering empiric Low-Dose Aspirin and LMWH to patients with unexplained RPL provides no therapeutic benefit, unnecessarily increases bleeding risks, and is explicitly unrecommended.
5.2
2. Rational Rationale for Progesterone Supplementation
Progesterone therapy is not a universal solution for early pregnancy maintenance and must not be prescribed indiscriminately to every patient with a history of miscarriage. Instead, vaginal or oral progesterone supplementation must be strictly reserved for a highly specific clinical presentation: patients presenting with active vaginal bleeding in the first trimester who also have a documented history of recurrent pregnancy loss. Outside of this specific scenario, routine empiric progesterone use provides no statistically significant improvement in live birth rates.
5.3
3. Absolute Avoidance of Experimental Immunomodulators
Because a significant portion of RPL cases remain unexplained, various costly immunomodulatory therapies have been utilized empirically. Clinicians must actively avoid experimental immunomodulators—including Intravenous Immunoglobulin (IVIG), intralipid infusions, and systemic corticosteroids—outside of formal, randomized clinical trials. These therapies carry significant systemic risks, have high financial costs, and lack robust clinical evidence confirming their efficacy in treating recurrent pregnancy loss.
6
Key Pearls & Takeaways
1 min•197 words
- Action at Two Losses: Do not delay the clinical workup until a third miscarriage occurs. Initiate a comprehensive diagnostic evaluation immediately after two consecutive pregnancy losses.
- The Mandatory Diagnostic Duo: Every recurrent pregnancy loss workup must include 3D uterine imaging to evaluate structural anatomy and a full serological panel for Antiphospholipid Syndrome.
- Halt the Routine Thrombophilia Panel: Inherited thrombophilia screening is expensive and provides no clinical utility in the routine management of RPL. Reserve these tests for patients with an independent history of deep vein thrombosis or systemic embolism.
- Limit Aspirin and LMWH to Proven APS: Dual antithrombotic therapy with low-dose aspirin and LMWH is a powerful tool, but it must be reserved strictly for laboratory-confirmed Antiphospholipid Syndrome. It has no place in the management of unexplained RPL.
- Progesterone Requires Bleeding + History: Do not prescribe progesterone universally. Restrict its use to patients who present with active first-trimester bleeding paired with a documented history of recurrent pregnancy loss.
- Reassure the Unexplained: When a comprehensive diagnostic workup reveals no identifiable cause, provide reassurance. With protocolized supportive care alone, couples with unexplained RPL achieve a successful live birth rate of 65% to 75%.
- The Mandatory Diagnostic Duo: Every recurrent pregnancy loss workup must include 3D uterine imaging to evaluate structural anatomy and a full serological panel for Antiphospholipid Syndrome.
- Halt the Routine Thrombophilia Panel: Inherited thrombophilia screening is expensive and provides no clinical utility in the routine management of RPL. Reserve these tests for patients with an independent history of deep vein thrombosis or systemic embolism.
- Limit Aspirin and LMWH to Proven APS: Dual antithrombotic therapy with low-dose aspirin and LMWH is a powerful tool, but it must be reserved strictly for laboratory-confirmed Antiphospholipid Syndrome. It has no place in the management of unexplained RPL.
- Progesterone Requires Bleeding + History: Do not prescribe progesterone universally. Restrict its use to patients who present with active first-trimester bleeding paired with a documented history of recurrent pregnancy loss.
- Reassure the Unexplained: When a comprehensive diagnostic workup reveals no identifiable cause, provide reassurance. With protocolized supportive care alone, couples with unexplained RPL achieve a successful live birth rate of 65% to 75%.
0/13