1
Introduction
1 min•154 words
Acute Chest Syndrome is a life-threatening, acute pulmonary complication that occurs in individuals with Sickle Cell Disease. It is defined clinically by the presence of a new pulmonary infiltrate on a chest radiograph involving at least one complete lung segment, accompanied by thoracic symptoms such as fever, cough, tachypnea, respiratory distress, or new-onset hypoxemia.
Among pediatric patients with Sickle Cell Disease, Acute Chest Syndrome stands as the second most common reason for hospital admission, closely following vaso-occlusive pain crises. More critically, it represents the leading cause of intensive care unit admission and the primary cause of premature mortality in this patient collective. While it can strike at any age, the highest incidence occurs in young pediatric patients between two and nine years of age. In a nine-year-old child, the clinical course can deteriorate with alarming speed, shifting from a simple localized bone pain crisis to full-scale, multi-lobar respiratory failure within a matter of hours.
Among pediatric patients with Sickle Cell Disease, Acute Chest Syndrome stands as the second most common reason for hospital admission, closely following vaso-occlusive pain crises. More critically, it represents the leading cause of intensive care unit admission and the primary cause of premature mortality in this patient collective. While it can strike at any age, the highest incidence occurs in young pediatric patients between two and nine years of age. In a nine-year-old child, the clinical course can deteriorate with alarming speed, shifting from a simple localized bone pain crisis to full-scale, multi-lobar respiratory failure within a matter of hours.
2
Background & Pathophysiology
2 min•208 words
The pathophysiology of Acute Chest Syndrome is complex, multifactorial, and characterized by a vicious, self-perpetuating cycle of microvascular occlusion, tissue ischemia, and severe inflammatory cascades within the lungs.
The primary initiating triggers in pediatric populations include pulmonary infections, bone marrow fat embolism secondary to a vaso-occlusive bone crisis, or localized pulmonary infarction from intravascular sickling. Common infectious pathogens identified in nine-year-old children include atypical bacteria like Mycoplasma pneumoniae and Chlamydia pneumoniae, respiratory viruses such as Respiratory Syncytial Virus, Influenza, and Adenovirus, and encapsulated bacteria like Streptococcus pneumoniae.
Regardless of the initial trigger, the final common pathway involves the sickling of deoxygenated erythrocytes within the low-velocity pulmonary microvasculature. Deoxygenated sickle hemoglobin polymerizes, causing the red blood cells to lose their elasticity and assume a rigid, crescent shape. These sickled cells express high levels of adhesion molecules, causing them to stick to the vascular endothelium and to each other, forming microvascular plugs.
This process leads to localized hypoxia, which further accelerates hemoglobin polymerization and deepens the sickling process. Concurrently, localized ischemia prompts a massive release of pro-inflammatory cytokines, causing endothelial dysfunction, alveolar edema, and a ventilation-perfusion mismatch. If left unchecked, this localized tissue injury propagates throughout the lung parenchyma, leading to widespread atelectasis, progressive respiratory failure, and acute cor pulmonale.
The primary initiating triggers in pediatric populations include pulmonary infections, bone marrow fat embolism secondary to a vaso-occlusive bone crisis, or localized pulmonary infarction from intravascular sickling. Common infectious pathogens identified in nine-year-old children include atypical bacteria like Mycoplasma pneumoniae and Chlamydia pneumoniae, respiratory viruses such as Respiratory Syncytial Virus, Influenza, and Adenovirus, and encapsulated bacteria like Streptococcus pneumoniae.
Regardless of the initial trigger, the final common pathway involves the sickling of deoxygenated erythrocytes within the low-velocity pulmonary microvasculature. Deoxygenated sickle hemoglobin polymerizes, causing the red blood cells to lose their elasticity and assume a rigid, crescent shape. These sickled cells express high levels of adhesion molecules, causing them to stick to the vascular endothelium and to each other, forming microvascular plugs.
This process leads to localized hypoxia, which further accelerates hemoglobin polymerization and deepens the sickling process. Concurrently, localized ischemia prompts a massive release of pro-inflammatory cytokines, causing endothelial dysfunction, alveolar edema, and a ventilation-perfusion mismatch. If left unchecked, this localized tissue injury propagates throughout the lung parenchyma, leading to widespread atelectasis, progressive respiratory failure, and acute cor pulmonale.
3
Clinical Features
2 min•234 words
The clinical presentation of Acute Chest Syndrome in a nine-year-old child can be deceptive, often starting with non-specific symptoms that mimic simple pneumonia or an isolated vaso-occlusive pain crisis.
History taking must focus heavily on the evolution of symptoms. The child frequently presents with a history of severe, progressive chest wall pain, back pain, or abdominal pain. This pain often causes splinting, where the child takes shallow breaths to avoid discomfort. Associated symptoms include a dry or productive cough, progressive shortness of breath, and high-grade fevers. It is highly common for a nine-year-old child to have been admitted initially for a vaso-occlusive pain crisis in the limbs, only to develop respiratory symptoms twenty-four to forty-eight hours later.
Physical examination reveals a child in respiratory distress. Key clinical signs include tachypnea, where the respiratory rate exceeds thirty breaths per minute for a nine-year-old, intercostal and subcostal retractions, nasal flaring, and grunting.
Auscultation of the lungs may reveal decreased breath sounds, localized crackles, rales, or bronchial breathing, typically over the lung bases. However, it is a vital clinical pearl that the physical examination of the chest can be completely normal early in the disease course. New-onset hypoxemia, demonstrated by a drop in peripheral oxygen saturation below ninety-two percent on room air, or a drop of more than three percent from the patient's baseline, is a profound and highly sensitive clinical indicator of impending Acute Chest Syndrome.
History taking must focus heavily on the evolution of symptoms. The child frequently presents with a history of severe, progressive chest wall pain, back pain, or abdominal pain. This pain often causes splinting, where the child takes shallow breaths to avoid discomfort. Associated symptoms include a dry or productive cough, progressive shortness of breath, and high-grade fevers. It is highly common for a nine-year-old child to have been admitted initially for a vaso-occlusive pain crisis in the limbs, only to develop respiratory symptoms twenty-four to forty-eight hours later.
Physical examination reveals a child in respiratory distress. Key clinical signs include tachypnea, where the respiratory rate exceeds thirty breaths per minute for a nine-year-old, intercostal and subcostal retractions, nasal flaring, and grunting.
Auscultation of the lungs may reveal decreased breath sounds, localized crackles, rales, or bronchial breathing, typically over the lung bases. However, it is a vital clinical pearl that the physical examination of the chest can be completely normal early in the disease course. New-onset hypoxemia, demonstrated by a drop in peripheral oxygen saturation below ninety-two percent on room air, or a drop of more than three percent from the patient's baseline, is a profound and highly sensitive clinical indicator of impending Acute Chest Syndrome.
4
Diagnosis & Workup
2 min•281 words
A definitive diagnosis of Acute Chest Syndrome requires a high index of clinical suspicion combined with diagnostic imaging and laboratory investigations.
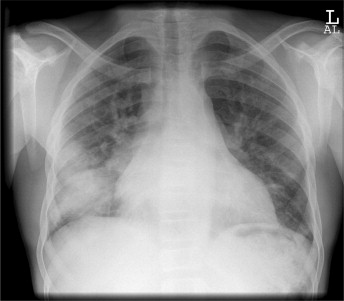
1. Imaging Studies: A chest radiograph is mandatory for any child with Sickle Cell Disease who presents with a fever or respiratory symptoms. The diagnostic hallmark is a new, distinct pulmonary infiltrate or consolidation. In children, these infiltrates are frequently localized to the lower lobes or may present as middle lobe syndrome. It is clinically crucial to realize that radiographic changes often lag behind physical findings. A clear chest radiograph taken at the onset of chest pain does not rule out the condition; images must be repeated if respiratory distress worsens.
2. Hematological Investigations: A complete blood count typically demonstrates a profound leukocytosis, which can track above twenty thousand cells per microliter, driven by intense systemic inflammation or underlying infection. There is often a significant drop in the hemoglobin concentration from the patient's steady-state baseline, reflecting accelerated hemolysis within the trapped pulmonary vasculature. The reticulocyte count remains highly elevated, confirming an active bone marrow response, though a sudden drop could warn of an aplastic crisis.
3. Markers of Hemolysis and Inflammation: Lactate dehydrogenase levels rise significantly, serving as a direct marker of intravascular hemolysis and pulmonary tissue injury.
4. Microbiology: Blood cultures and sputum cultures must be collected promptly to isolate bacterial pathogens. Sputum or nasopharyngeal swabs should undergo polymerase chain reaction testing to screen for atypical bacteria and common respiratory viruses.
5. Monitoring and Blood Gas Analysis: Continuous pulse oximetry is mandatory. An arterial blood gas analysis is indicated in severe distress to monitor for respiratory acidosis, track the partial pressure of oxygen, and calculate the alveolar-arterial oxygen gradient.
1. Imaging Studies: A chest radiograph is mandatory for any child with Sickle Cell Disease who presents with a fever or respiratory symptoms. The diagnostic hallmark is a new, distinct pulmonary infiltrate or consolidation. In children, these infiltrates are frequently localized to the lower lobes or may present as middle lobe syndrome. It is clinically crucial to realize that radiographic changes often lag behind physical findings. A clear chest radiograph taken at the onset of chest pain does not rule out the condition; images must be repeated if respiratory distress worsens.
2. Hematological Investigations: A complete blood count typically demonstrates a profound leukocytosis, which can track above twenty thousand cells per microliter, driven by intense systemic inflammation or underlying infection. There is often a significant drop in the hemoglobin concentration from the patient's steady-state baseline, reflecting accelerated hemolysis within the trapped pulmonary vasculature. The reticulocyte count remains highly elevated, confirming an active bone marrow response, though a sudden drop could warn of an aplastic crisis.
3. Markers of Hemolysis and Inflammation: Lactate dehydrogenase levels rise significantly, serving as a direct marker of intravascular hemolysis and pulmonary tissue injury.
4. Microbiology: Blood cultures and sputum cultures must be collected promptly to isolate bacterial pathogens. Sputum or nasopharyngeal swabs should undergo polymerase chain reaction testing to screen for atypical bacteria and common respiratory viruses.
5. Monitoring and Blood Gas Analysis: Continuous pulse oximetry is mandatory. An arterial blood gas analysis is indicated in severe distress to monitor for respiratory acidosis, track the partial pressure of oxygen, and calculate the alveolar-arterial oxygen gradient.
5
Management
3 min•403 words
The management of Acute Chest Syndrome in a nine-year-old child demands an immediate, aggressive, and highly coordinated multidisciplinary approach. Treatment must be initiated concurrently with the diagnostic workup.
Respiratory Support and Oxygenation: Supplemental oxygen must be administered immediately to maintain target oxygen saturations above ninety-five percent. This is critical because hypoxemia directly drives red blood cell sickling. If progressive respiratory distress or worsening hypoxemia occurs despite high-flow nasal cannula or a non-rebreather mask, non-invasive positive pressure ventilation, such as continuous positive airway pressure, must be implemented early. This helps recruit atelectatic alveoli and reduces the work of breathing. Mechanical ventilation is reserved for severe, refractory respiratory failure.
Empiric Antimicrobial Therapy: Because infection is a primary trigger and cannot be immediately differentiated from infarction, broad-spectrum antimicrobial therapy must be started within one hour of presentation. The standard regimen includes an intravenous third-generation cephalosporin, such as Ceftriaxone, to cover encapsulated organisms, combined with an oral or intravenous macrolide, such as Azithromycin, to provide mandatory coverage for atypical pathogens.
Judicial Fluid Management: Intravenous fluid management requires a careful balancing act. Dehydration must be avoided as it increases blood viscosity and promotes sickling. However, fluid overload is equally dangerous, as it directly precipitates pulmonary edema and worsens alveolar hypoxia. Fluids should be maintained strictly at one to one point five times the maintenance rate, using hypotonic or isotonic solutions, with frequent reassessment of the child's fluid balance and breath sounds.
Aggressive Pain Management and Incentive Spirometry: Providing adequate analgesia is essential to prevent hypoventilation and subsequent atelectasis. Intravenous opioids, such as Morphine, are commonly required. Pain management must be titrated carefully to relieve suffering without causing respiratory depression. Alongside analgesia, the use of incentive spirometry is a cornerstone of therapy. A nine-year-old child must be coached to perform ten deep breaths every one to two hours while awake to keep the alveoli open.
Transfusion Therapy: Blood transfusion is a definitive, disease-modifying therapy for Acute Chest Syndrome. A simple packed red blood cell transfusion is indicated if the hemoglobin drops significantly below the patient's baseline and the disease is mild to moderate. However, if the child shows signs of severe respiratory distress, multi-lobar involvement, or refractory hypoxemia, an emergent automated or manual Exchange Transfusion must be performed. The goal of exchange transfusion is to rapidly lower the fraction of sickle hemoglobin to below thirty percent while optimizing the oxygen-carrying capacity of the blood without increasing overall blood viscosity.
Respiratory Support and Oxygenation: Supplemental oxygen must be administered immediately to maintain target oxygen saturations above ninety-five percent. This is critical because hypoxemia directly drives red blood cell sickling. If progressive respiratory distress or worsening hypoxemia occurs despite high-flow nasal cannula or a non-rebreather mask, non-invasive positive pressure ventilation, such as continuous positive airway pressure, must be implemented early. This helps recruit atelectatic alveoli and reduces the work of breathing. Mechanical ventilation is reserved for severe, refractory respiratory failure.
Empiric Antimicrobial Therapy: Because infection is a primary trigger and cannot be immediately differentiated from infarction, broad-spectrum antimicrobial therapy must be started within one hour of presentation. The standard regimen includes an intravenous third-generation cephalosporin, such as Ceftriaxone, to cover encapsulated organisms, combined with an oral or intravenous macrolide, such as Azithromycin, to provide mandatory coverage for atypical pathogens.
Judicial Fluid Management: Intravenous fluid management requires a careful balancing act. Dehydration must be avoided as it increases blood viscosity and promotes sickling. However, fluid overload is equally dangerous, as it directly precipitates pulmonary edema and worsens alveolar hypoxia. Fluids should be maintained strictly at one to one point five times the maintenance rate, using hypotonic or isotonic solutions, with frequent reassessment of the child's fluid balance and breath sounds.
Aggressive Pain Management and Incentive Spirometry: Providing adequate analgesia is essential to prevent hypoventilation and subsequent atelectasis. Intravenous opioids, such as Morphine, are commonly required. Pain management must be titrated carefully to relieve suffering without causing respiratory depression. Alongside analgesia, the use of incentive spirometry is a cornerstone of therapy. A nine-year-old child must be coached to perform ten deep breaths every one to two hours while awake to keep the alveoli open.
Transfusion Therapy: Blood transfusion is a definitive, disease-modifying therapy for Acute Chest Syndrome. A simple packed red blood cell transfusion is indicated if the hemoglobin drops significantly below the patient's baseline and the disease is mild to moderate. However, if the child shows signs of severe respiratory distress, multi-lobar involvement, or refractory hypoxemia, an emergent automated or manual Exchange Transfusion must be performed. The goal of exchange transfusion is to rapidly lower the fraction of sickle hemoglobin to below thirty percent while optimizing the oxygen-carrying capacity of the blood without increasing overall blood viscosity.
6
Key Pearls & Takeaways
1 min•178 words
- Time is Tissue: Acute Chest Syndrome can progress with terrifying speed. Do not wait for a chest radiograph to worsen if a nine-year-old sickle cell patient develops new hypoxemia or respiratory distress. Begin aggressive therapy immediately.
- The Splinting Hazard: Severe chest or abdominal pain causes shallow breathing, which directly leads to lung atelectasis, localized hypoxia, and a full-blown pulmonary sickling crisis. Always optimize pain management and enforce incentive spirometry every hour.
- The Dual Antibiotic Mandate: Standard pneumonia protocols are insufficient. Every patient with suspected Acute Chest Syndrome requires a third-generation cephalosporin plus a macrolide to ensure atypical pathogens are effectively covered.
- Transfusion Choice: A simple transfusion is useful for mild drops in hemoglobin, but severe respiratory distress or multi-lobar consolidations demand an urgent exchange transfusion to lower the sickle hemoglobin percentage below thirty percent.
- Fluid Precision: Avoid the extremes. Never over-hydrate a child with Acute Chest Syndrome, as the injured pulmonary vasculature leaks easily, causing fluid overload and severe pulmonary edema. Keep fluids tightly regulated between one and one point five times maintenance.
- The Splinting Hazard: Severe chest or abdominal pain causes shallow breathing, which directly leads to lung atelectasis, localized hypoxia, and a full-blown pulmonary sickling crisis. Always optimize pain management and enforce incentive spirometry every hour.
- The Dual Antibiotic Mandate: Standard pneumonia protocols are insufficient. Every patient with suspected Acute Chest Syndrome requires a third-generation cephalosporin plus a macrolide to ensure atypical pathogens are effectively covered.
- Transfusion Choice: A simple transfusion is useful for mild drops in hemoglobin, but severe respiratory distress or multi-lobar consolidations demand an urgent exchange transfusion to lower the sickle hemoglobin percentage below thirty percent.
- Fluid Precision: Avoid the extremes. Never over-hydrate a child with Acute Chest Syndrome, as the injured pulmonary vasculature leaks easily, causing fluid overload and severe pulmonary edema. Keep fluids tightly regulated between one and one point five times maintenance.
0/6
